A 54 year old post menopausal lady presented with a small 1.5 cm size suspicious BIRADS IV lesion in breast on routine screening mammography (Fig -1). US Guided Biopsy was reported as ductal hyperplasia.
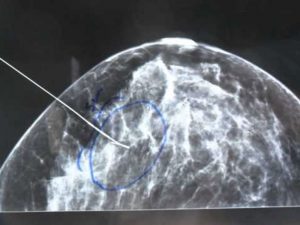
US guided FNAC was suggestive of papillary neoplasm. The lesion was small and deep seated and could not be felt on breast examination. On the day of surgery a radiopaque wire was placed in the centre of the lesion under ultrasound guidance (Fig – 2).

The patient was next shifted to operation theatre and under general anaesthesia, the tissue around the wire was excised (Fig – 3)

Specimen was sent for specimen mammography to assess completeness of excision (Fig – 4 & 5).


Pathological assessment during surgery with frozen section was done and was negative for malignancy. Final Histopathology was reported as Atypical Ductal Hyperplasia.
The patient did not require any further surgery and asked to undergo annual screening mammography and clinical breast examination.